
Gestational Diabetes
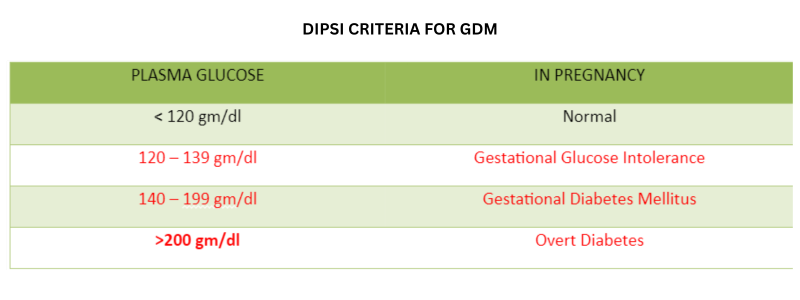
DIPSI CRITERIA FOR GDM
IF OGTT value is more then 140 then you need to be investigated further. (Fbs,PP2BS,Hb1AC) Ref. DIPSI : DIABETES IN PREGNANCY STUDY GROUP OF INDIA GDM : GESTATIONAL DIABETES MELLITUS. FOR MORE DETAILS KINDLY VISIT : DIPSI CRITERIA FOR GDM
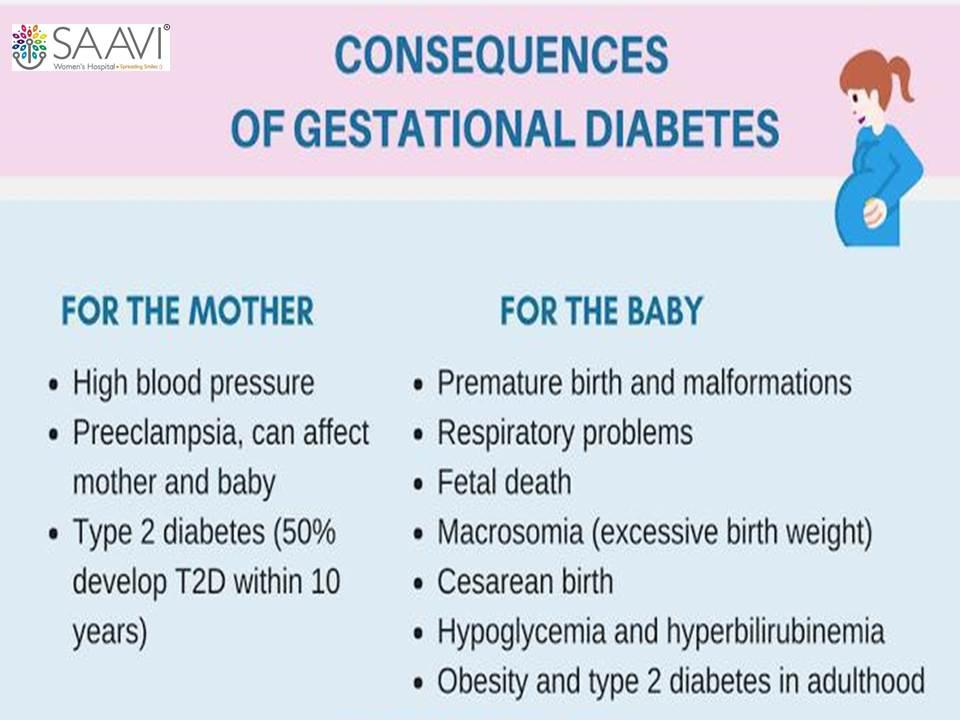
Consequnces of Gestational Diabetes

Risk of Macrosomia in baby

Estimated Fetal Wight Chart

BMI-graph
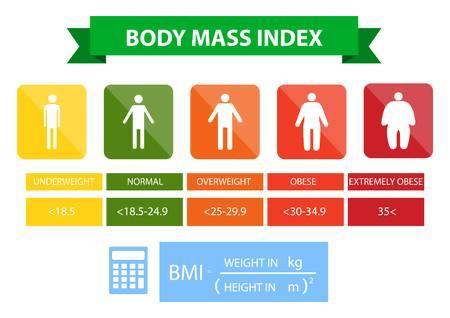
BMI



THE INFORMATION ON THIS WEBSITE IS OBTAINED THROUGH ONLINE SOURCES AND MEDICAL LITERATURE. IT'S NOT MEANT TO REPLACE AN ACTUAL CONSULTATION WITH A DOCTOR BUT IS A STARTING POINT FOR YOUR OWN RESEARCH.

