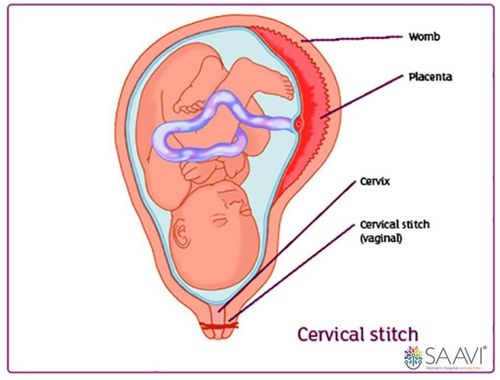
A cervical stitch
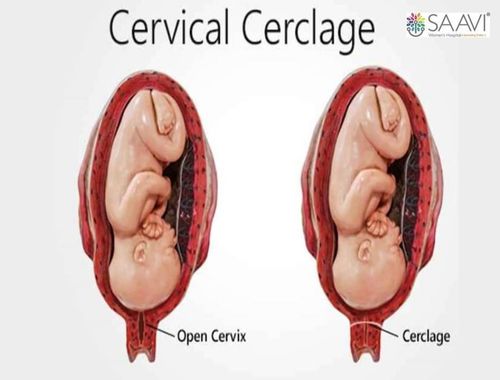
Cervical Cerclage
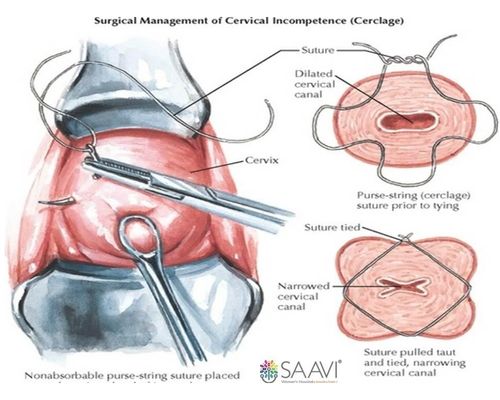
The transvaginal cervical stitch procedure (left) and once it is completed (right)



THE INFORMATION ON THIS WEBSITE IS OBTAINED THROUGH ONLINE SOURCES AND MEDICAL LITERATURE. IT'S NOT MEANT TO REPLACE AN ACTUAL CONSULTATION WITH A DOCTOR BUT IS A STARTING POINT FOR YOUR OWN RESEARCH.

